我们的转运专家!从新生儿到成人





通信主板选项适用于:

在您的移动设备上通过 Hamilton Connect 应用访问呼吸数据。它提供了旨在促进和简化通气工作流程的工具。







Various solutions are available for all the main types of helicopters and ambulances, as well as for hospital beds, stretchers, surfaces, shelves, poles, rails, and ceilings.
With four different types of handles and multiple mounts, the HAMILTON-T1 is a portable ventilator that adapts to your specific environment and situation.

如果您必须执行 CPR,则 CPR 通气自适应通气设置。其显示与情况相关的主要监测参数和曲线,并通过快速访问可预配置的设置、适当的报警和触发调节以及 CPR 计时器显示来支持您的工作流程。
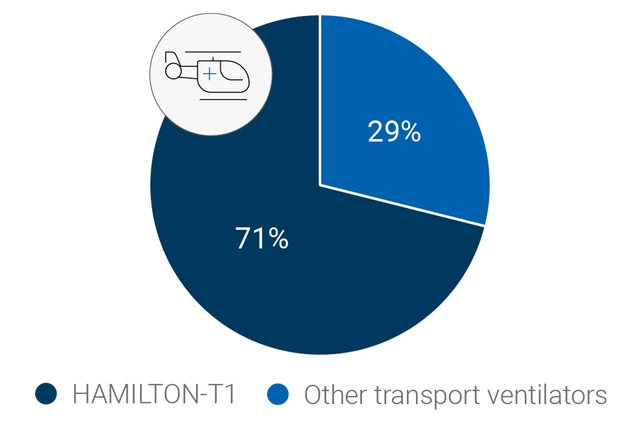
As a transport ventilator for ambulances, helicopters, and more, the HAMILTON-T1 is a favorite for many rescue crews. According to the HOVER survey (

Ventilators suitable for pandemics and mass casualties must be versatile and meet various requirements. The HAMILTON-T1 meets or exceeds all requirements in the AARC Guidelines for Acquisition of Ventilators to Meet Demands for Pandemic Flu and Mass Casualty Incidents (
Discover the HAMILTON-T1 from every angle and click on the hotspots to learn more.
| 病人组 | 成人/儿童、新生儿 |
|---|---|
| 外形尺寸(宽x深x高) | 320 x 220 x 270 mm(呼吸机主机) 630 x 630 x 1380 mm(无手柄) 630 x 630 x 1433 mm(带手柄) |
| 重量 | 6.5 kg(14.3 磅) 18.5 kg(40.8 磅)(含台车) |
| 监视器尺寸和分辨率 | 214 mm(8.4 英寸)对角线 640 x 480 像素 |
| 可拆卸式监视器 | |
| 电池运行时间 | 一块电池 4 小时 两块电池 8 小时 |
| 热插拔电池 | |
| 气源 | 集成涡轮 |
| O2 接头 | DISS (CGA 1240) 或 NIST |
| 连接 | CO2/护士呼叫器/COM1,二氧化碳/SpO2/COM1,二氧化碳/SpO2/湿化器和 COM1,USB 端口,RJ-45 以太网端口 |
| 音量 | 43 dB(在正常运行情况下) |
| 容量控制、流量控制 | |
|---|---|
| 定量、适应性压力控制 | |
| 智能通气 | ASV®、INTELLiVENT®-ASV®(选项) |
| 无创通气 | |
| 高流量 | |
| 肺力学指标可视化(动态肺) | |
|---|---|
| 病人呼吸机依赖性可视化 | |
| 食道压测量 | |
| 二氧化碳图 | |
| 氧饱和度监测 |
| 肺复张性评估和肺复张 (P/V Tool Pro) | |
|---|---|
| 人机同步 (IntelliSync+) | |
| CPR 通气 | |
| Hamilton Connect 模块 |
| 远程连接至 HAMILTON-H900 湿化器 | |
|---|---|
| 集成 IntelliCuff 气囊压力控制器 | |
| 集成气动雾化器 | |
| 集成 Aerogen 雾化器 | |
| 与 Sedaconda ACD-S 麻醉剂输送系统的兼容性 |

使命召唤
暴露于极端环境意味着军用呼吸机必须满足非常特殊的要求。这是 HAMILTON-T1 的用途所在。
根据病人的肺力学指标和呼吸用力,ASV 通气模式每天 24 时从插管到拔管连续调整每次呼吸时的呼吸频率、潮气量和吸气时间。
INTELLiVENT-ASV 智能通气模式持续调整病人的通气和氧合状态。
它根据临床医生设定的目标值和病人的生理输入设置分钟通气量、PEEP 和氧浓度。
集成气动雾化器完全与吸气和呼气时间同步。
集成同步 Aerogen 雾化系统作为一个选配件提供 (
输送药物气溶胶粒子的细水雾有助于您恢复支气管痉挛、提高通气效率和减少高碳酸血症 (
近端流速和二氧化碳测量使我们的呼吸机能生成最新的容积二氧化碳图,为评估通气质量和新陈代谢活动提供生要依据。
通气状态面板显示与病人的呼吸机依赖性相关的六个参数,包括氧合状态、CO2 清除状态和病人活动。
各栏中上下移动的浮动指示器显示给定参数的当前值。
通过独特的呼吸机连接选项可以直接从呼吸机的显示屏上操作 HAMILTON-H900 湿化器(
湿化器也可以根据所选的通气模式自动选择湿化模式(有创、无创或高流量)。
高流量鼻导管治疗(
说话瓣膜选项让气管切开的病人说话,而且允许他们甚至在接受通气治疗时吞咽。
调节呼吸机的监测、触发和报警管理,以在压力控制模式 (PCV+, SPONT, PSIMV+) 下与说话瓣膜兼容。
快速撤机是 INTELLiVENT-ASV 模式的一个功能,其可提供对病人状况的持续动态监测和控制,从而评估病人是否适于拔管。
动态肺面板向您显示下列重要监测数据的实时图表视图:
呼吸机可根据所选的监测参数组合显示动态环图。有了趋势图功能,您可以看到针对您选择的监测参数和时间框所显示的趋势数据。
设备持续将监测参数保存在其存储器中,即使在待机时也不停止。
氧饱和度选项提供集成无创氧饱和度测量,数据方便地显示在您的呼吸机上。
我们还提供氧饱和度传感器的全面组合方案。
无创通气模式提供压力支持流速切换的自主呼吸(NIV 和 NIV-ST 模式)和压力控制时间切换的指令呼吸 (NIV-ST)。
与使用压缩空气的呼吸机相比,我们的涡轮驱动呼吸机能够提供更高的峰值流量。这就保证了即便漏气严重也具有最佳性能。
nCPAP 模式的设计使您仅需设置期望的持续气道正压。之后,根据病人状况和潜在漏气调整流速。这就防止了意外峰值压力的产生,保证了高效的漏气补偿,并帮助减少了氧气消耗。由于压力测量灵敏度很高,流速的调整非常迅速。



美国犹他州盐湖城
Intermountain Life Flight 是犹他州领先的空中救援服务。自 1978 年开始计划以来,我们信守承诺,通过直升机、固定翼和地面救护车为患者提供卓越护理。
Zürich, Schweiz
Swiss Air-Rescue 是瑞士空中救援的非营利私人基金会,由瑞士救生协会成员于 1952 年成立,总部设在苏黎世机场。
美国明尼苏达州布卢明顿市
Life Link III 运营着遍布明尼苏达州和威斯康星州的九个直升机基地。全天候提供直升机和飞机服务,提供现场应急响应和机构间转运。

Our preassembled breathing circuit sets include the essential consumables to operate the ventilator, conveniently packaged in one single bag.
All our essential consumables are specially developed for Hamilton Medical ventilators with guaranteed manufacturer quality.

To manage ventilation you usually have to set multiple parameters, such as pressure, volume, inspiratory and expiratory triggers, cuff pressure, and more. And each time your patient's condition changes, you have to make one or even several readjustments.
To simplify this process and reduce the knob-turning, we have created a range of solutions:
Adaptive Support Ventilation (ASV) is a ventilation mode that provides continuous adaptation of respiratory rate, tidal volume, and inspiratory time, depending on the patient’s lung mechanics and effort. ASV has been shown to shorten the duration of mechanical ventilation in various patient populations with fewer manual settings (
Conventional solutions for cuff pressure management require you to monitor and adjust cuff pressure by hand.
IntelliCuff secures your patient’s airway (

Whenever there is a problem, the ventilator alerts you using the alarm lamp, sound, and message bar.
The on-screen help offers you suggestions on how to resolve the alarm.

Our online Academy offers easy-to-follow learning paths to familiarize you with Hamilton Medical products and technologies as quickly as possible.



我们使用 HAMILTON-T1 为院内转运和院外转运病人通气。保证病人转运过程中的通气质量与床头通气质量等同。
跨学科儿科 ICU 高级医生
Center for Pediatrics and Adolescent Medicine,德国美因茨
能够将 nCPAP 与 HAMILTON‑T1 结合使用是我们的一大优点。某些幼儿转运时不再需要插管。
Life Flight 新生儿呼吸科护士
Intermountain Life Flight,美国犹他州盐湖城
HAMILTON‑T1 呼吸机小巧而紧凑,但仍具备常频 ICU 呼吸机的所有特点。
Rega Jet 护士长
Rega - Swiss Air Rescue,瑞士苏黎世

We are constantly working on further evolving our products. New features are added and existing features improved to ensure you always have access to the latest ventilation technology over your ventilator’s lifetime.


Whether it is in the ICU, in the MRI suite, or during transport, the user interface of all Hamilton Medical ventilators works in the same way.
Our Ventilation Cockpit integrates complex data into intuitive visualizations.
We develop our accessories for the highest possible patient safety and ease of use in mind. Whenever possible, we integrate them with our ventilators to simplify operation of the complete ventilator system.

我们的通气极客团队很乐意帮助您选择最适合您临床护理环境的通气设备,并帮助您实现治疗目标。获取个性化报价或安排电话回访,了解更多信息。