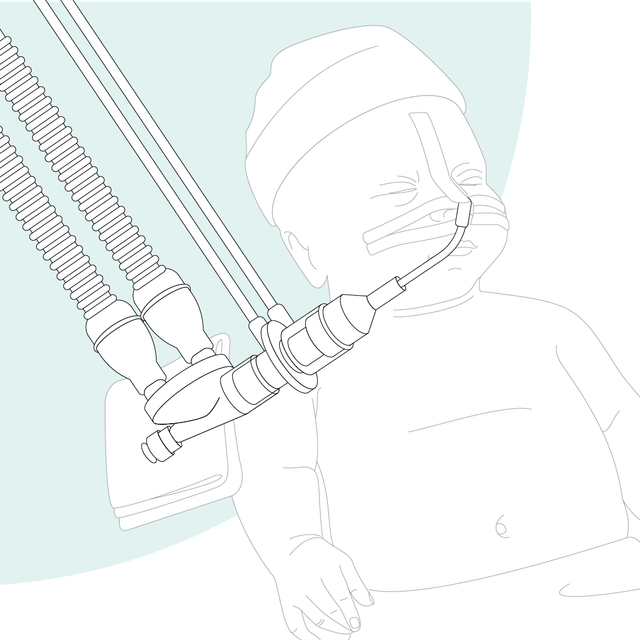
从 1983 年,近端流量传感器一直是我们呼吸机的中心部件。整个通气过程依赖流量传感器的测量和准确度,而且他们提供气道开口的数据。
精确的容量、流量和压力数据对进行正确诊断和避免通气设置不当的常见副作用至关重要。同时还依靠它实现我们的一些高级技术,例如 ASV 和 INTELLiVENT-ASV 模式、IntelliSync+ 及 P/V Tool。

我们的呼吸机可测量病人气道附近的流量和压力。研究表明,通气病人的潮气量应通过放置在气管插管的流量传感器来进行测定 (

准确测定呼出潮气量 (VTE) 至关重要 (
对于您的优点:
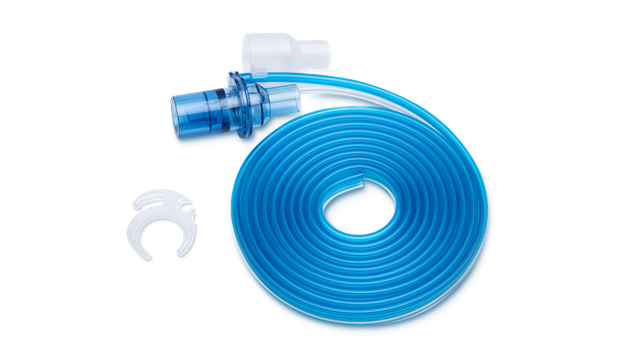
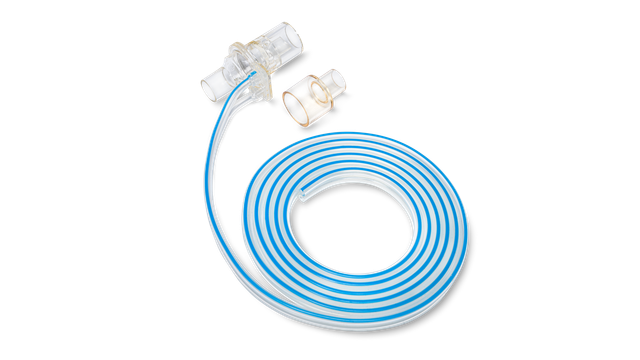
我们提供适用于成人、儿童及新生儿病人的 Hamilton Medical 哈美顿医疗公司耗材。您可根据您的机构政策选择可重复使用产品或一次性产品。

Hamilton Medical 哈美顿医疗公司一次性流量传感器帮助我们防止交叉污染,因为我们没有必要担心在另一名病人身上重复使用流量传感器。
呼吸治疗主任(直至 2018 年)
美国德克萨斯州拉伯克大学医疗中心