作者: Justin Seemueller, Respiratory Clinical Specialist, Sentara Norfolk General Hospital
日期: 24.02.2021
It is a generally accepted practice to limit tidal volume (per IBW), plateau pressure, and driving pressure (Plat-PEEP) within acceptable ranges for lung-protective ventilation (
Gattinoni et al. have utilized derivative formulas to estimate mechanical power as a metric to mitigate lung damage. The most accurate bedside method is complicated and requires clinicians to perform an inspiratory hold to measure plateau pressure for accurate resistance and elastance values (
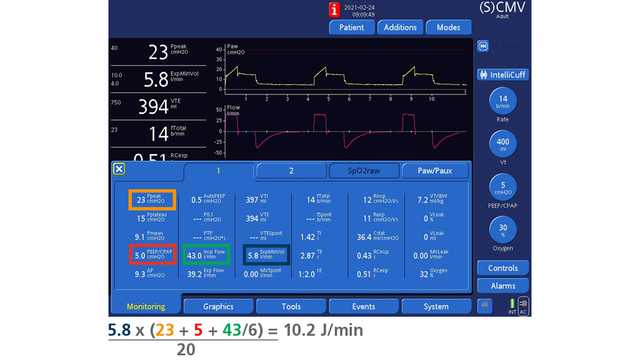
Simplified methods have recently emerged to quickly estimate mechanical power without the need for an inspiratory hold maneuver. Gattinoni et al. proposed an acceptably accurate method for Volume Control ventilation; the simplified method was validated by comparing animal experimentation with a cohort of ICU patients from seven previously published studies (
These new methodologies are interesting in the context of modern electronic medical record (EMR) systems, some of which can apply formulas to device integrated ventilator data. Epic is a fairly ubiquitous EMR system, and the company's system analysts have confirmed that it is possible to automatically calculate these types of shortened mechanical power formulas within new flowsheet rows. This presents an exciting prospect for generating instantaneous reports on all ventilator patients within a hospital system, who are currently receiving what might be considered unsafe levels of mechanical power. In two separate observational cohorts, a value of 17 J/min or greater was associated with a higher risk of death (