

作者: Justin Seemueller, Respiratory Clinical Specialist, Sentara Norfolk General Hospital
日期: 24.02.2021
Data currently suggests that a MP of 17.0 J/min is associated with higher risk of death (
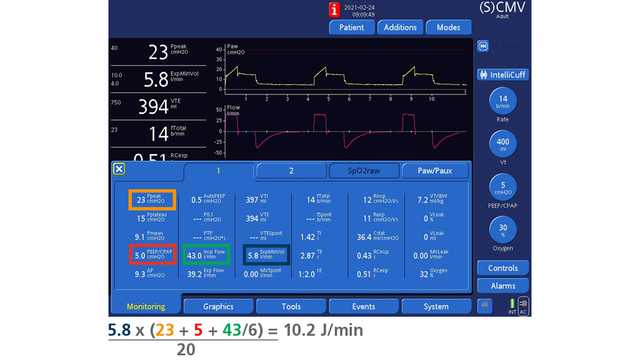
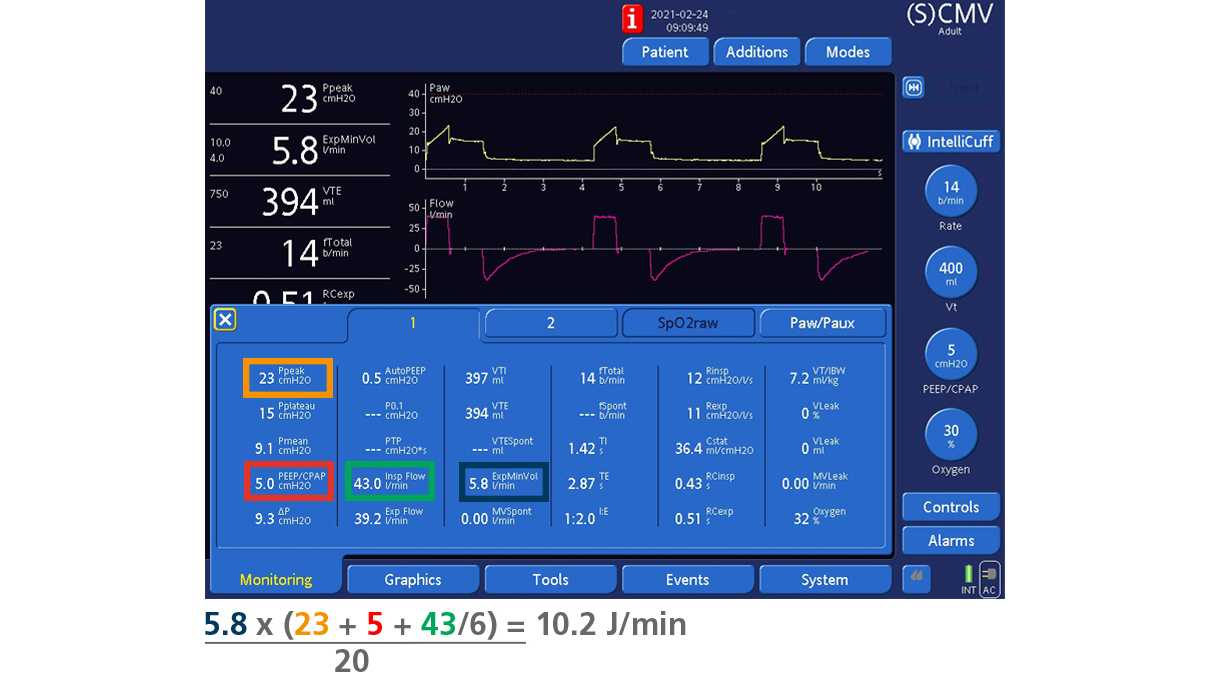
Powersurr.corr = [VE x (Peak Pressure + PEEP + F/6)] / 20
If we use the corresponding values shown in the ventilator's Monitoring window, the equation is as follows:
Powersurr.corr = [ExpMinVol x (Ppeak + PEEP/CPAP + Insp Flow/6)] / 20
Figure 1 below shows the calculation using the corresponding values as shown in the Monitoring window.
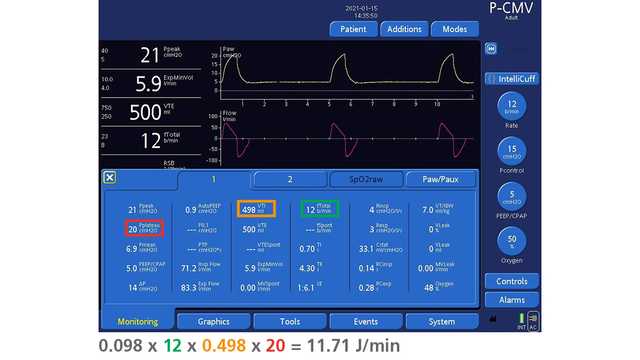
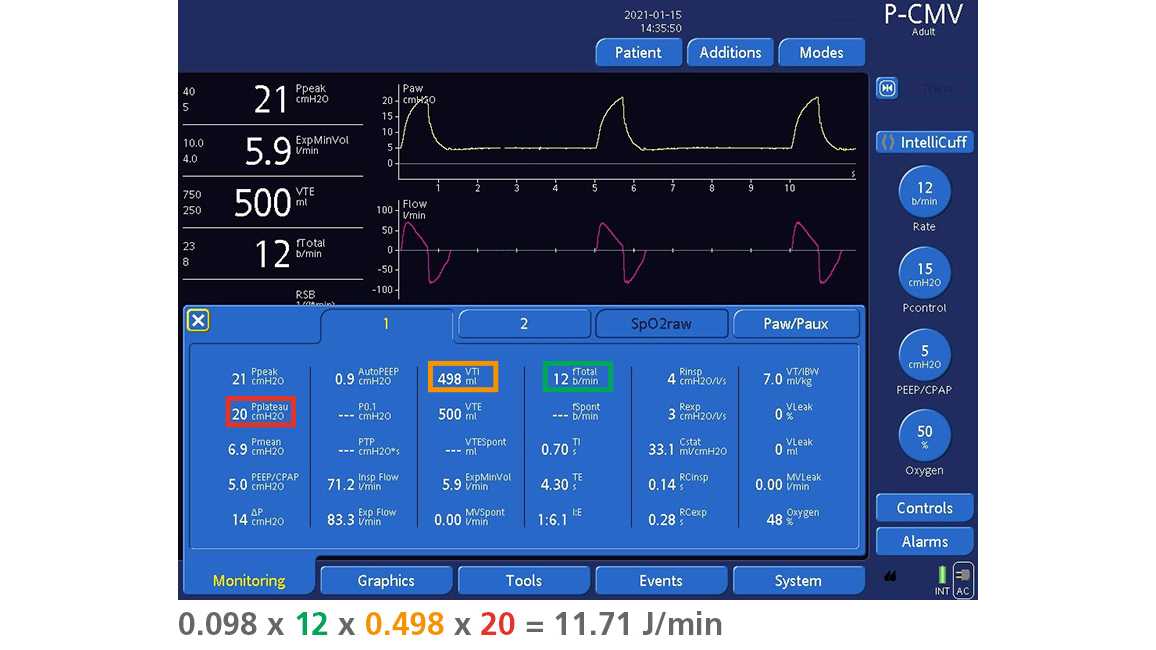
Below is a simplified method of calculating mechanical power in Pressure Control proposed by Van der Meijden et al. and Becher et al. (
MPPCV = 0.098 x RR x VT x (∆Pinsp + PEEP)
It is possible to further simplify their formula by replacing "∆Pinsp + PEEP” with plateau pressure, as they are equivalent by definition. Pplateau can be measured by means of an inspiratory hold (available in the Tools window). Alternatively, an estimated value of Pplateau is displayed in the Monitoring window of Hamilton Medical ventilators. If we use the corresponding values as shown in the Monitoring window, the equation is as follows:
MPPCV = 0.098 x fTotal x VTI x Pplateau
Figure 2 below shows the calculation using the corresponding values as shown in the Monitoring window.
These formulas may assist in identifying mechanically ventilated patients in need of earlier intervention.