



Wir helfen Ihnen gerne und werden Ihre Anfrage so schnell wie möglich beantworten.

Zugang zu allen Dokumenten, Videos, Artikeln, E-Learning-Modulen und weiteren Ressourcen zu all unseren Produkten.

Herkömmliche Lösungen für das Cuff-Druck-Management erfordern, dass Sie den Cuff-Druck von Hand überwachen und einstellen.
Um die gewünschten Cuff-Druck-Bereiche jederzeit aufrechtzuerhalten, können täglich bis zu acht manuelle Anpassungen erforderlich sein (

IntelliCuff sichert die Atemwege Ihres Patienten (
Sie können ihn entweder als eigenständiges Gerät für alle Beatmungsgeräte oder als integrierte Lösung für den HAMILTON-C6 und den HAMILTON-G5/S1 verwenden.

Sie stellen einfach den gewünschten Cuff-Druck ein und IntelliCuff übernimmt die kontinuierliche Überwachung und Aufrechterhaltung des eingestellten Drucks. Der im Cuff gemessene Druck wird als Monitoring-Wert angezeigt.
Im Falle eines beschädigten Cuffs löst IntelliCuff einen Alarm aus und kompensiert die Leckage, um den Atemweg sicher zu halten.

Wir setzen IntelliCuff bei maschinell beatmeten Patienten als Standardfunktion ein, um VAP zu vermeiden. IntelliCuff kontrolliert den Cuff-Druck automatisch und regelmässig. Das ist eine grosse Hilfe für uns Pflegekräfte, da wir den Druck nicht jede Stunde manuell überprüfen müssen.
Stationsleiterin Intensivpflege
Kantonsspital Graubünden, Chur, Schweiz
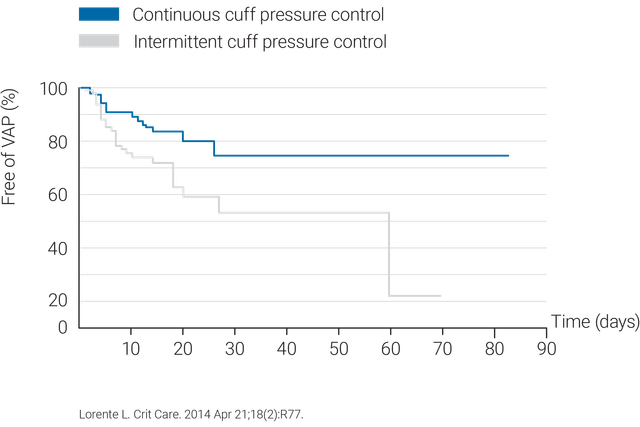
Die Verwendung eines kontinuierlichen Cuff-Druck-Kontrollsystems wie IntelliCuff ist effektiver bei der Aufrechterhaltung des Cuff-Drucks innerhalb eines optimalen Bereichs (
Um Verletzungen der Trachea und Druckgeschwüre zu vermeiden, ist der Cuff-Druck beim IntelliCuff standardmässig auf 25 cmH2O eingestellt (

IntelliCuff ist als eigenständiges Gerät für alle Beatmungsgeräte oder als integrierte Lösung verfügbar; beim HAMILTON-C6 und HAMILTON-G5 als Option und beim HAMILTON-S1 als Standardfunktion.





