




The well-trained eye of a ventilation expert is capable of detecting asynchronies by analyzing the shapes of the flow and pressure waveforms.
However, the patient’s condition can change from breath to breath and the expert cannot always be at the bedside.
That is where IntelliSync+ takes over. This technology mimics the expert‘s eye to identify signs of patient effort (trigger) or relaxation (cycling) on the waveform.
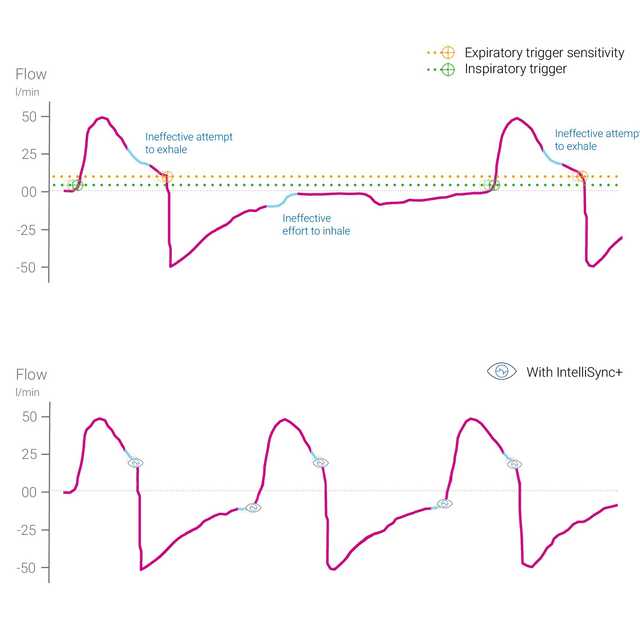
IntelliSync+ continuously analyzes waveform signals at least one hundred times per second. This enables IntelliSync+ to detect patient efforts immediately and to initiate inspiration and expiration in real time, thus replacing conventional trigger settings for inspiration and expiration.
For maximum flexibility, you can choose to activate IntelliSync+ for either the inspiratory trigger or the expiratory trigger, or both.

A high number of major patient-ventilator asynchronies occur in around 25% of all mechanically ventilated patients (
Analyzing waveform shapes is a reliable, accurate, and reproducible method for assessing patient-ventilator interaction. Automation of this method may allow continuous monitoring of ventilated patients and/or improved breath-triggering and cycling (
Mojoli F, Orlando A, Bianchi IM, et al.
A recent study showed that automated control of ventilator cycling off based on real time analysis of waveforms provided a reliable means of improving synchronization in mechanically ventilated patients.


IntelliSync+ is a completely noninvasive method that does not require any additional hardware or accessories. Simply activate the option on your ventilator to use it in invasive or noninvasive ventilation modes on adult and pediatric patients.
As IntelliSync+ can also be combined with conventional triggers, you can choose to use IntelliSync+ either during inspiration, expiration, or both.


Our asynchrony reference card gives you an overview of the most common asynchrony types, their causes, and how to detect them.
IntelliSync+ is available as an option on the HAMILTON-C6 and HAMILTON-G5.
