

Author: Clinical Experts Group, Hamilton Medical
Date of first publication: 14.07.2017
Last change: 30.09.2020
(Originally published 14.07.2017) Previously: select Exp hold, when flow=0 select Exp hold again to deactivate hold maneuver. SW versions updated.In the presence of dynamic pulmonary hyperinflation, the average end-expiratory pressure inside the alveoli (i.e., the actual, total PEEP (PEEPtot)) is higher than the PEEP applied by the ventilator (PEEPe). The difference between PEEPtot and PEEPe corresponds with the intrinsic PEEP (PEEPi), and is also known as AutoPEEP (1).
AutoPEEP may also be referred to as air-trapping, breath stacking, dynamic hyperinflation, inadvertent PEEP, or occult PEEP.
AutoPEEP is a common phenomenon in mechanically ventilated patients with long expiratory time constants (RCexp), for example patients with chronic obstructive pulmonary disease or acute severe asthma.
IMPORTANT: The resulting AutoPEEP cannot be seen on the airway pressure curve shown on the ventilator’s screen during normal breath delivery.
(Figure 1 below: Source Garcia Vicente et al. (
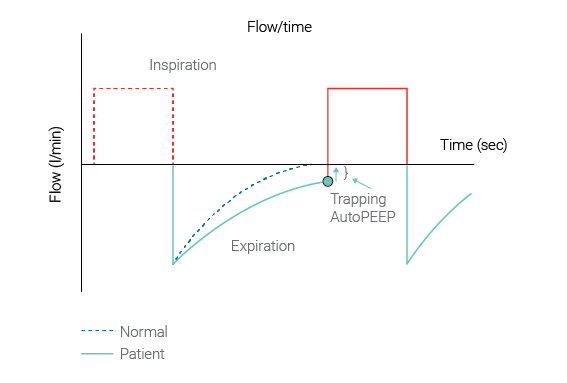
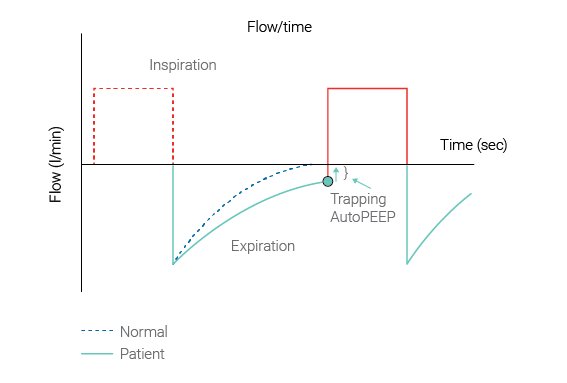
AutoPEEP predisposes the patient to increased work of breathing, barotrauma, hemodynamic instability and difficulty in triggering the ventilator. Failure to recognize the hemodynamic consequences of AutoPEEP may lead to inappropriate fluid restriction or unnecessary vasopressor therapy. AutoPEEP can potentially interfere with weaning from mechanical ventilation.
Caregivers should monitor whether AutoPEEP is occurring during ventilation, and set their ventilation control parameters accordingly to avoid the negative consequences of AutoPEEP.
All Hamilton Medical Ventilators have the unique capability of showing AutoPEEP as a monitoring parameter on a breath-by-breath basis. It is calculated using the LSF method applied to the entire breath (
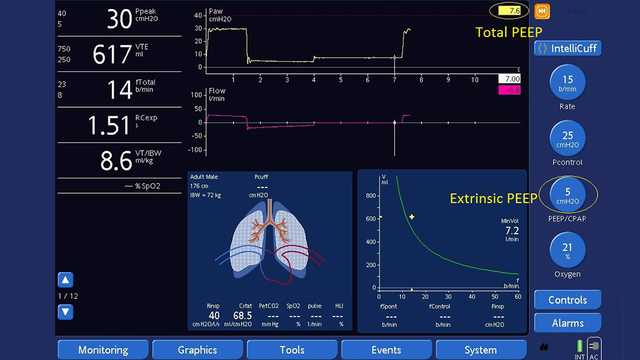
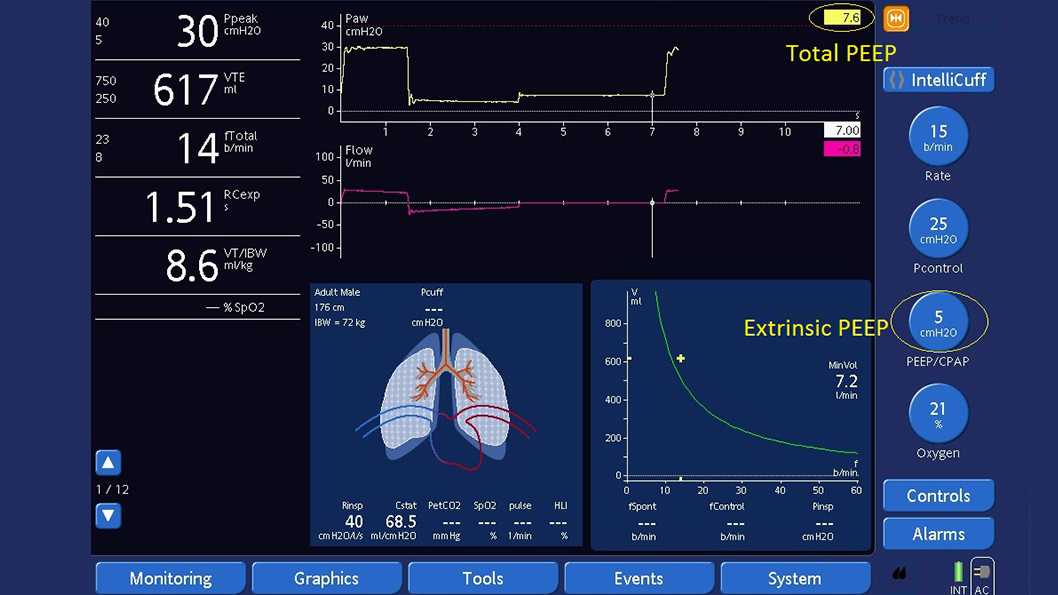
Measuring the total PEEP with an expiratory hold maneuver (see Figure 2 below):
Ensure the Paw waveform is displayed.
| AutoPEEP | = total PEEP - extrinsic PEEP = intrinsic PEEP |
|---|---|
| PEEP | = extrinsic PEEP and is preselected |
| Total PEEP | = intrinsic PEEP + extrinsic PEEP |
If AutoPEEP is present unintentionally, caregivers should consider adapting the control parameters to avoid air-trapping by increasing the exhalation time. Use of large-diameter endotracheal tubes, bronchodilators, short inspiratory times, long expiratory times, lower respiratory rates and the use of sedatives can be necessary to avoid the dynamic hyperinflation caused by air-trapping.
All Hamilton Medical ventilators feature the intelligent ventilation mode Adaptive Support Ventilation (ASV®). ASV automatically employs lung-protective strategies to minimize complications from AutoPEEP.
Relevant devices: HAMILTON-G5/S1 (sw v2.8x and later); HAMILTON-C3 (sw v2.0.x and later), HAMILTON-C6 (sw v1.1.x and later)
See full citation for (