

Author: Süha Demirakca
Date of first publication: 07.11.2019
However over-inflation, particularly over a prolonged period, may limit mucosal perfusion. The standard cuff pressure to provide leakage-free ventilation is usually set at 25 mbar. Absence of leakage is primarily essential in special situations such as during a recruitment maneuver. In all other circumstances, common practice in many PICU`s is to keep the cuff inflated to provide minimal leakage at peak inspiratory pressure, so that cuff pressure can usually be down-titrated to values between 20–25 mbar.
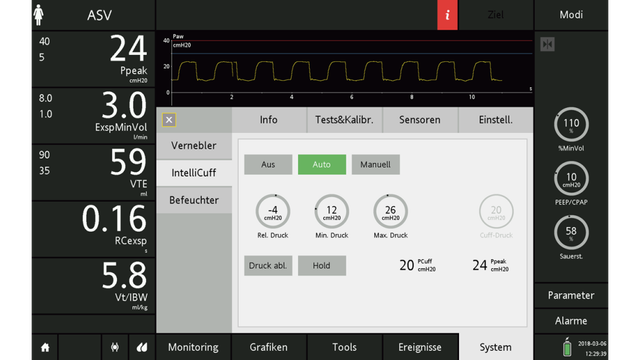
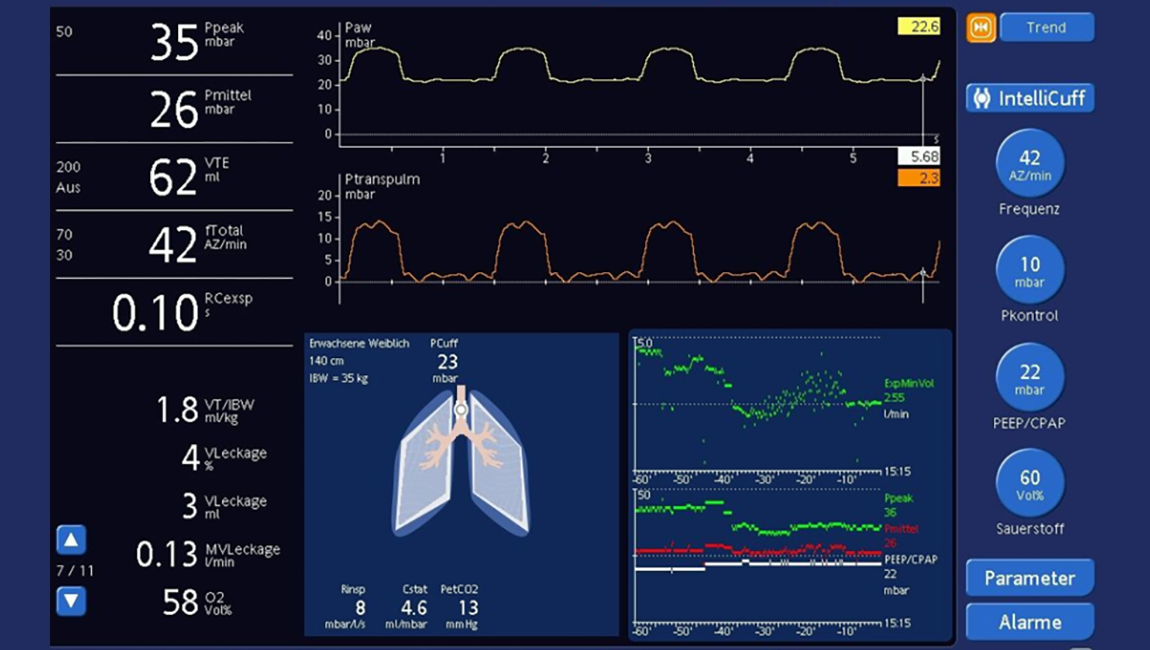
Cuff pressure leak thresholds in children will vary with sedation status and positioning of the patient, and are also influenced by coughing and suctioning. Pressure drops occur within a few hours after manual adjustment of the cuff pressure. Therefore, regular monitoring of the cuff pressure to provide accurate cuff pressure control is very important. This can be best achieved with an online cuff controller tool such as Intellicuff.
A pre-extubation leak pressure test may provide information about the risk of a subglottic upper airway obstruction occurring. Because the cuff is located in the subglottic area, the cuff leak pressure threshold appears to measure subglottic edema. A simple method of gaining this information is to test whether an audible leak occurs at a peak inspiratory pressure of 25 mbar, after the patient has been suctioned and the cuff has been deflated. The presence of an audible pre-extubation leak at 25 mbar indicates that no subglottic upper airway obstruction will occur, whereas the absence of leak at 25 mbar signals a subglottic stenosis that will need treatment in 18%–19% of patients. The importance of leakage in the case of cuffed endotracheal tubes may be related to the fact that in comparison to uncuffed tubes, the cuffed tubes used are usually smaller because the cuff can be inflated to maintain tidal volume and pressure.
Full citataions see below: