





Conventional solutions for cuff pressure management require you to monitor and adjust cuff pressure by hand.
You could need as many as eight manual adjustments daily to maintain desired cuff pressure ranges at all times (

IntelliCuff secures your patient’s airway (
You can use it either as a standalone device for all mechanical ventilators or as an integrated solution for the HAMILTON-C6 and the HAMILTON-G5/S1.

You just set your desired cuff pressure, then IntelliCuff takes over and continuously monitors and maintains that set pressure. The pressure measured in the cuff is displayed as a monitoring value.
In the event of a damaged cuff, IntelliCuff generates an alarm and keeps compensating for the leak to keep the airway secure.

We use IntelliCuff as a standard feature to help prevent VAP in mechanically ventilated patients. IntelliCuff controls the cuff pressure automatically and regularly. This is a great help for us caregivers since we don’t have to check the cuff pressure manually every hour.
Head of ICU Nursing Department
Grisons Cantonal Hospital, Chur, Switzerland
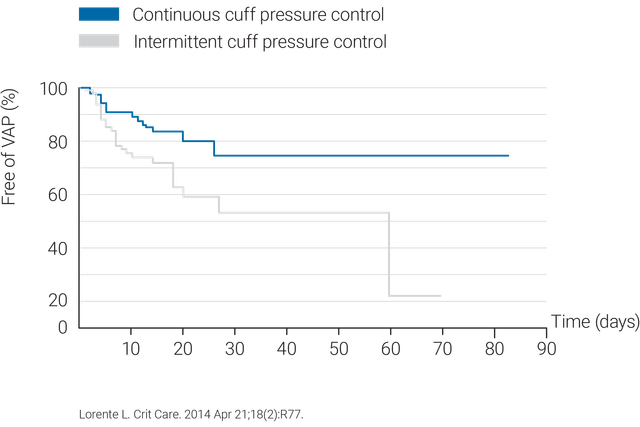
The use of a continuous cuff pressure control system such as IntelliCuff is more effective in maintaining cuff pressure within an optimal range (
To avoid tracheal injuries and pressure ulcers, IntelliCuff has a default cuff pressure set at 25 cmH2O (

IntelliCuff is available as a standalone device for all ventilators or as an integrated solution that is optional on the HAMILTON-C6 and HAMILTON-G5, and standard on the HAMILTON-S1.





