Wir helfen Ihnen gerne und werden Ihre Anfrage so schnell wie möglich beantworten.

Wenn Sie Unterstützung benötigen, stehen Ihnen unser Team weltweit sowie unsere Experten vor Ort zur Verfügung. Wir freuen uns über Ihr Feedback: es hilft uns, zu wachsen.

Zugang zu allen Dokumenten, Videos, Artikeln, E-Learning-Modulen und weiteren Ressourcen zu all unseren Produkten.

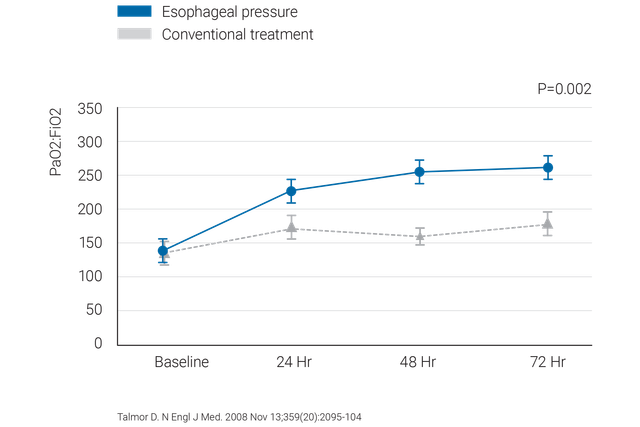
Die Messung des ösophagealen Drucks (Pes) ist eine minimalinvasive Monitoring-Methode, mit der der transpulmonale Druck bestimmt werden kann.
Die gängigste Methode zur Messung des Pes ist die Verwendung eines luftgefüllten Ballons, der in einen Ösophaguskatheter integriert ist.
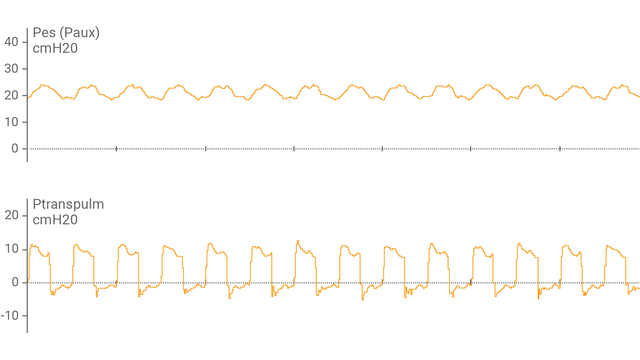
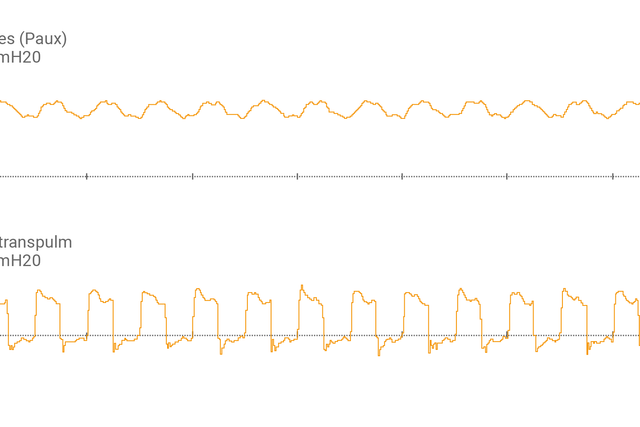
Nachdem Sie den Ösophagusballonkatheter an den Hilfsanschluss angeschlossen und die korrekte Platzierung bestätigt haben, zeigt der Bildschirm des Beatmungsgerätes den Ösophagusdruck (Pes) und die transpulmonalen Druckwerte (Ptranspulm) als Kurven an.
Sie können den statischen Ptranspulm mit inspiratorischen und exspiratorischen Hold-Manövern messen.

Zur Beurteilung der Rekrutierbarkeit und zur Durchführung von Recruitmentmanövern kann der transpulmonale Druck auch in Kombination mit dem P/V Tool® verwendet werden.

Sehen Sie sich diese kurze Demonstration an, um zu verstehen, wie Sie mit dem transpulmonalen Druck-Monitoring den PEEP genauer einstellen können.


Bewährte Empfehlungen aus der klinischen Praxis, wie Sie bei der Verwendung des ösophagealen Drucks bei ARDS-Patienten vorgehen und was Sie vermeiden sollten.
Wir bieten ösophageale Ballonkatheter von CooperSurgical und nasogastrale NutriVent-Katheter.
Das transpulmonale Druck-Monitoring zählt zur Standardausstattung bei den Beatmungsgeräten HAMILTON-C6 und HAMILTON-G5/S1.