

Autor: Simon Franz
Datum: 11.06.2020
While the ambient pressure drops with the height above sea level, a closed system such as an ETT cuff keeps its absolute pressure constant. This results in a relative pressure increase of the ETT cuff pressure compared to the environment. Many endotracheal tube (ETT) cuffs are therefore over-inflated during air transport, potentially causing pressure-related tracheal injuries. Weisberg et al. (2017) discovered that there is no linear relationship between ETT cuff pressures and maximum altitude during transports near sea level (up to an altitude of 3,000 ft). Their results support routine monitoring of ETT cuff pressures, as many cuffs were initially over-inflated. However, there appears to be no need to replace air with saline at altitudes near sea level (
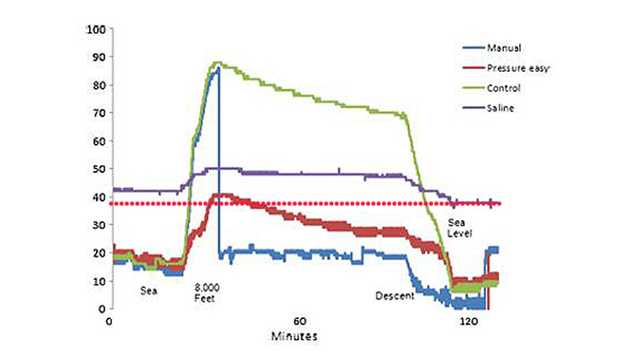
For information about this behavior at higher altitudes, such as in the pressurized cabin of a fixed-wing airplane (8,000 ft), we can refer to the work of Britton et al. (2014). They compared four different methods of managing endotracheal cuff pressure, and evaluated the pressure at sea level (baseline) and 8,000 ft (see Figure 1). They showed that filling the cuff with saline did not prevent the cuff pressure from increasing with higher altitudes (
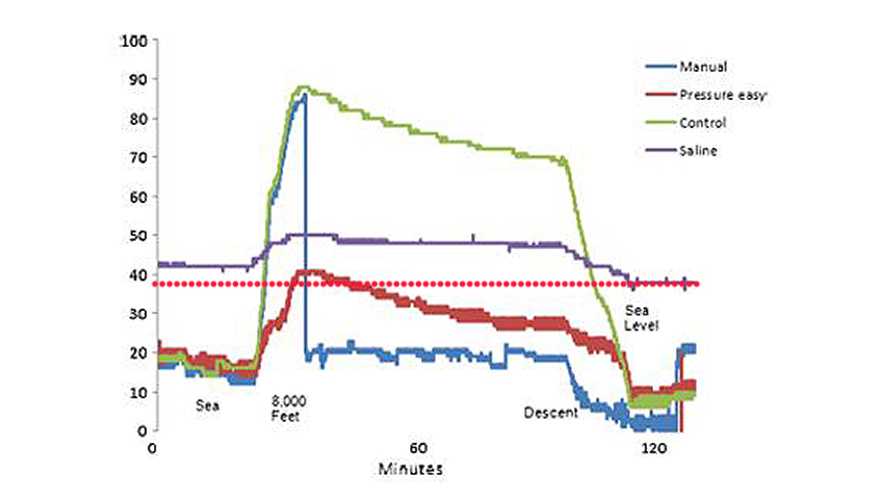
It is generally accepted that the potential harmful effects of a cuffed endotracheal tube are due to transmural pressures between the cuff and tracheal mucosa, which exceed the capillary perfusion pressure of the tissue. Using saline instead of air does not provide sufficient protection against these high pressures, and also affects the ability to measure the actual cuff pressure. From a pathophysiological view, it therefore makes much more sense to control the pressure rather than the volume in the cuff.
With the automatic cuff-pressure controller, IntelliCuff®, Hamilton Medical offers a solution for automatic measurement and maintainence of cuff pressure for all patient groups for critical care, interhospital transport, and anesthesia.